Light Before Air: The Photobiomodulation Paradox
Why oxygen therapy fails when the cell door is locked. The mechanism of Cytochrome C Oxidase and the crucial role of red light as a primer.
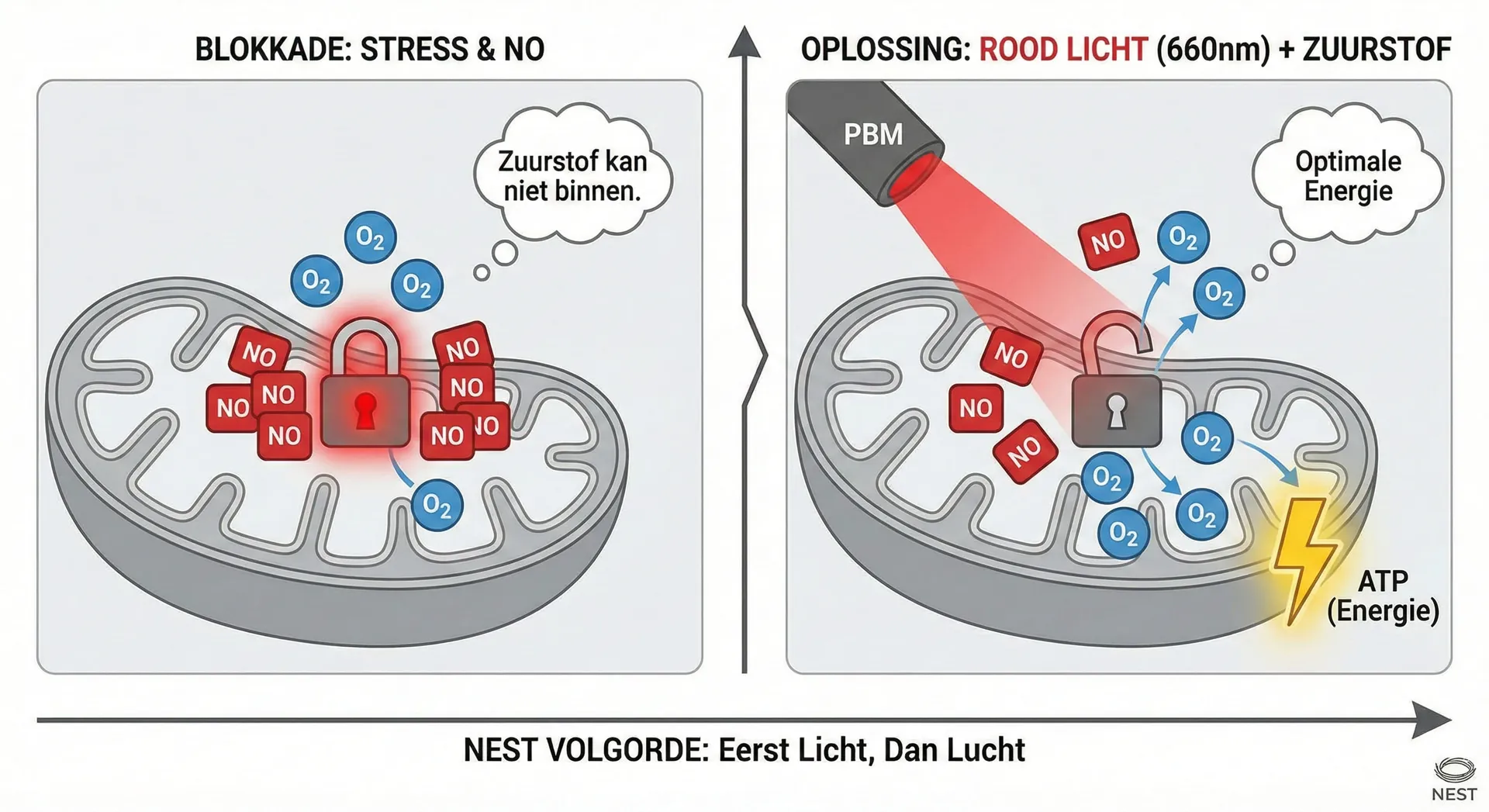
- Nitric oxide (NO) blocks oxygen uptake in stressed cells.
- Red light (660nm) breaks this blockade, allowing the cell to 'breathe' again.
- HBOT sessions are 30-40% more effective when preceded by PBM.
Imagine: you are trying to fill your car with fuel, but the fuel cap is locked. It does not matter how high the quality of the petrol is (or in our case: how pure the oxygen is); the engine receives nothing.
This is exactly what happens in a body under chronic stress or after surgery.
At NEST we maintain the rule: Light First, Then Air. This is not an aesthetic choice, but a biophysical necessity.
The Molecular Blockade
Within your cells are mitochondria, the power plants. Inside these plants runs a process called the Electron Transport Chain. The final step in this chain is managed by an enzyme: Cytochrome C Oxidase (CCO).
This enzyme has one task: bind oxygen and convert it to ATP (energy).
However, under stress, illness or ageing, your body produces an excess of Nitric Oxide (NO).
- Normally, NO is useful for vasodilation.
- But in excess, it competes with oxygen. It binds to the CCO receptor and blocks it.
The result: The cell ‘suffocates’ at a molecular level, even when you breathe normally. This is called mitochondrial dysfunction.
The Key: 660nm Wavelength
This is where Photobiomodulation (PBM) comes in. Specifically, red light with a wavelength of 660 nanometres has a unique property: it is absorbed by the CCO enzyme.
The energy of the photons (light particles) is precisely sufficient to break the bond between the nitric oxide and the receptor. This is called photodissociation.
- The red light hits the cell.
- The harmful NO is displaced.
- The receptor is free again.
The NEST Sequence
This explains why simply booking an oxygen session is inefficient. If we placed you directly in the NEST HBOT laboratory without preparation, a large proportion of that precious oxygen would be unable to enter your cells due to the NO blockade.
By first applying 15-20 minutes of red light therapy (Phase 1: Priming):
- Clear: We remove the blockade.
- Load: Only then do you enter the oxygen chamber (Phase 2: Potentiation).
- Result: The oxygen finds an ‘open door’ and can be directly converted into recovery energy.
This is the difference between superficial intervention (pleasant for a moment) and bio-engineering (measurable result).
Clinical Specifications: Not All Red Light Is Equal
Many clients arrive at NEST with this assumption: they have already tried red light at home. They purchased a ‘therapeutic lamp’, sat under it for months, and saw no result. They assume photobiomodulation simply does not work for them.
This is a common misconception. What they attempted was not clinical photobiomodulation. It was consumer-grade equipment.
The Two Wavelength Windows
Clinical PBM operates at two primary wavelength windows, and both are necessary:
660nm (Visible Red) This wavelength penetrates only 2-3 millimetres into tissue. It reaches the dermis (skin layer) and underlying muscle tissue. This is where you must remove nitric oxide (NO) from superficial mitochondria—the mitochondria in your skin, your muscles, your local vascularity. For locally dysfunctional muscles, skin conditions, or muscle recovery, 660nm is your working spectrum.
850nm (Near-Infrared) This penetrates 3-5 centimetres. This reaches deep tissue, bone marrow, and crucially: the cerebral cortex through the skull. This is your channel for neural reactivation.
Both wavelength windows are essential. Using only one is like activating only half your circuit.
The Irradiance Threshold: The Difference Between Effect and Futility
Here is where it becomes critical. Many consumer devices advertise “red light therapy” but deliver biologically negligible irradiance (light intensity):
- Below 50mW/cm²: Effect is biologically negligible. This is what consumer helmets and panels deliver. Your cells do not “feel” this light.
- 50-100mW/cm²: Borderline. Possibly mild effects on very superficial tissue.
- 100-200mW/cm²: This is the therapeutic window. This reliably activates Cytochrome C Oxidase.
- 200-300mW/cm²: Still effective, but you approach the boundary of thermal overload.
- >300mW/cm²: The biphasic dose response reverses. Tissue heating overrides photobiomodulation. You burn rather than heal.
NEST’s Clinical Panels: Specification and Power
In our red light therapy laboratory, our clinical panels deliver 150mW/cm² at skin surface with total fluence of 60J/cm² per ten-minute session. This is not inexpensive equipment. This is calibrated for biological response.
By comparison: a standard consumer lamp? It delivers 5-20mW/cm². This can never achieve Cytochrome C Oxidase activation at therapeutic depth. You sit beneath an expensive light bulb that does nothing biologically.
The Precision of Dosage
This is why NEST clients see results and consumer users do not. It is not about “light” in the abstract. It is about precisely the correct wavelengths, precisely the correct intensity, precisely the correct duration and fluence. This is what pharmacological precision means in physical form.
A fifteen-minute PBM session at 150mW/cm² is not the same as “sitting under a consumer lamp for a month.” One is clinically active. The other is theatre. For practical experiences and insights from our clients see also our article on Red Light Therapy Experiences.

Scientific References
"Red-to-near-infrared light modulates oxygen consumption of isolated Cytochrome C Oxidase in the presence of a nitric oxide donor, supporting the photodissociation hypothesis."
"Photobiomodulation acts via absorption by Cytochrome C Oxidase, resulting in increased ATP production and mitochondrial signaling."